


'First Choice': How China and the WHO created mass ventilator hysteria
And harmed innocents along the way.

Mechanical ventilators have long been considered a last resort solution for treating patients with respiratory illness. The exact percentage varies, but the studies are unanimous in concluding that the vast majority of people who are put on a mechanical ventilator never make it off of one. In treating respiratory ailments, the highly invasive, high-risk maneuver that is mechanical ventilation is usually prefaced by less invasive measures, such as positive airway pressure machines like CPAP or BiPAP devices, or simple oxygen delivering nose prongs. But when COVID-19 hit, the long established scientific guidance on proper patient care was tossed out the window, along with other established norms, in the face of this much-hyped novel virus.
When the COVID-19 pandemic hit full swing, this learned and phased approach to ventilator use was nowhere to be seen. Doctors in Italy, Spain, and New York City in particular were rushing to mechanical ventilation early and often, thanks in part to a fear-based transmission threat and an “expert consensus” that originated in China & was broadcast far and wide by the World Health Organization (WHO).
In early March, when COVID-19 was ravaging western Europe and sounding alarm bells in the United States, the WHO released COVID-19 provider guidance documents to healthcare workers. Citing experience “based on current knowledge of the situation in China,” the WHO recommended mechanical ventilators as an early intervention for treating COVID-19 patients. The guidance recommended escalating quickly, if not immediately, to mechanical ventilation. In doing so, they cited the guidance being presented by Chinese medical journals, which published papers in January and February claiming that “Chinese expert consensus” called for “invasive mechanical ventilation” as the “first choice” for people with moderate to severe respiratory distress.


The WHO further justified this approach by claiming that the less invasive positive air pressure machines could result in the spread of aerosols, potentially infecting healthcare workers with the virus.

The aerosol spread problem, however, is more or less a very loose hypothesis. There remains questionable evidence that COVID-19 spreads through aerosols from airway pressure or oxygen devices. And there are established protocols for protecting medical workers from potential aerosol infection when using these devices.
“This is more theoretical fear than a real fear,” Dr. David Hill, a pulmonary and critical care specialist who has experience treating COVID-19 patients, and who is a spokesperson for the American Lung Association, told Time Magazine.
Seeing the situation in Wuhan unfold, and evaluating the guidance passed on from China and the WHO, U.S. “public health experts” became convinced that ventilators were an absolute necessity, and that we needed tens of thousands, if not hundreds of thousands more of these devices, to stave off the disease. Hysterical epidemiological modelers, the same ones that had just claimed millions of people were about to die from COVID-19 in the United States, took to claiming that there was a mass ventilator shortage in the United States. Governors across the country were now demanding ventilators by the boatload.

After much bipartisan insistence from Congress, the president ordered U.S. manufacturers to build ventilators under the Defense Production Act. Based on the Wuhan experience, the United States was taking China and the WHO at its word, and reorienting some of our private industry economic engines towards building medical devices.


Meanwhile, China, strangely, did not have much use for its ventilators anymore. China was now exporting ventilators in incredible quantities. Under the guise of humanitarian behavior, China was making a fortune off of manufacturing and exporting ventilators (many of which did not work correctly and even killed patients) around the world.


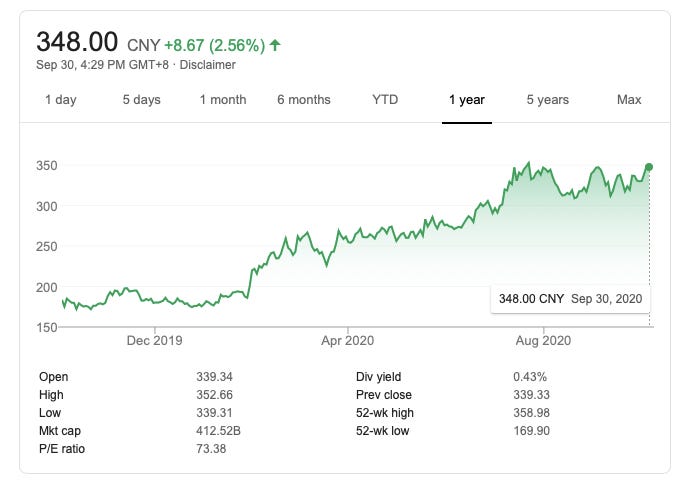
Mindray, China’s biggest publicly traded ventilator-producing company, saw an explosion in growth thanks to ventilator sales. The market cap for the business is up 100% since the beginning of the pandemic.
Meanwhile, as COVID-19 case growth exploded in New York City, some doctors began to notice that something was horribly wrong with the way patients were being treated for the disease. The COVID-19 guidance coming out of China, and being distributed in english by the World Health Organization, wasn’t working.
In New York City, early and often ventilator use became a common theme, and it had devastating consequences for infected patients caught in the middle of the hysteria.
On March 31, Dr. Cameron Kyle-Sidell, who had been caring for ICU patients at one of the hardest-hit hospitals in the city, sounded the alarm about the ventilator issue. He took to YouTube and became something of a ventilator whistleblower.
“We are operating under a medical paradigm that is untrue,” Dr. Kyle-Sidell explained. “I fear that this misguided treatment will lead to a tremendous amount of harm to a great number of people in a very short time.”
“I don’t know the final answer to this disease, but I’m quite sure that a ventilator is not it,” he continued. “This method being widely adopted at this very moment at every hospital in the country … is actually doing more harm than good.”
An April Reuters interview with dozens of medical specialists made it clear that mechanical ventilator overuse had become a global issue. “Many highlighted the risks from using the most invasive types of them - mechanical ventilators - too early or too frequently, or from non-specialists using them without proper training in overwhelmed hospitals,” the report said.

By May, it was common knowledge in the medical community that early ventilator use was hurting, not helping COVID-19 patients, and that less invasive measures were in fact very effective in assisting recoveries. However, by then, the damage had already been done.
The WHO recommendation has opened up a continuing conversation in the scientific community about the medical ethics of potentially unnecessarily harming a patient to hypothetically protect one’s colleagues from a virus (And one that is simply not that lethal. Although, in hindsight, it was difficult to be sure of this in early 2020).
The “early action” ventilator guidance from China, which was distributed to the world by the WHO, very likely resulted in many lives taken from us far too soon. To my knowledge, neither WHO nor the Chinese government (which controls its medical associations) has acknowledged this catastrophic misstep.

Amazing job. This is real and informative with back up figures and resources
Thank you
Great job in getting into the details of one of the reasons of this mass hysteria and subsequent deaths! Keep it up Jordan.